Products involved in the illegal pangolin trade can be grouped into three types: meat, scales and body parts. Pangolin scales account for a large portion of the reported illegal trade. Heinrich et al. (2017) summarised international confiscation reports from 2010 to 2015 and found that more than 55,000 kg of scales was confiscated during this period. If the average weight of scales on one pangolin is around 500 g (Challender & Waterman, 2017; Zhou, Zhao, Zhang, Wang, & Wang, 2012), these data indicate that more than 100,000 pangolins were trafficked from 2010 to 2015. China has been identified as one of the major demand countries, and Traditional Chinese Medicine (hereafter TCM) has been shown to be linked with illegal trade in pangolin scales through illegal products found in markets and shops (Xu, Guan, Lau, & Xiao, 2016; Yin, Meng, Xu, & Liu, 2015).
Traditional Chinese Medicine dates back more than 5,000 years and is still widely used today in China (Chen & Xie, 1999). In 2016, TCM hospitals and clinics treated 962 million patients in China, and medical services provided through TCM treatment accounted for 15.8% of the total medical service provided in that year (National Health & Family Planning Commission of the PRC, 2017; Tang, Liu, & Ma, 2008). The use of pangolin scales in TCM can be traced back to AD 480 when prescriptions containing this ingredient were documented in the Bencao jing jizhu, which was later cited in the famous Compendium of Materia Medica (Li, 1578).
In addition to illegal pangolin products found in TCM markets, a legal market for pangolin scale medicine also exists to support TCM use in China (Xing et al., 2020). Regulations specify that: (a) pangolin scales can be legally traded for medicinal purposes by 711 certified hospitals in China; (b) the quantities of scales that can be traded every year are regulated through a quota system assigned by the Forestry and Grassland Administration at different administrative levels; (c) certification is required to trade and farm pangolins or pangolin products, and manufacture pangolin products; before 2017, importation of African pangolins and their products was still allowed with appropriate certification, but thereafter all pangolin species were included in CITES Appendix I at CoP17 (Johannesburg, 2016) and importation was banned; (d) products from legal pangolin farms can be traded if relevant certification is issued. However, there is no evidence of successful commercial farming to date (Hua et al., 2015; Hu, 2016; Li, 2017). The only legal source of pangolin scales in the current TCM market in China is therefore the quota assigned by the Chinese government.
The pangolin scale quota system started in China in 2008. Sources of pangolin scales assigned in the quota included private-held or government-held stockpiles. Data on quotas assigned to the market are publicly available for the period 2008–2015. These data show that a total of 186,067 kg of pangolin scales were released to trade, with a mean annual quota of 26,581 ± 1,580 kg. [Corrections added on 7 November 2020, after first online publication: this sentence has been amended to reflect the correct average annual quota amounts]. The legal pangolin scale market is therefore of considerable size and requires similar levels of conservation attention to that focused on the general illegal scale trade. Even though large quantities of pangolin scales have been traded legally or illegally for TCM use, little attention has been paid to research in this area. This is particularly the case for TCM practitioners, who are key stakeholders in the pangolin scale trade since they are directly involved in using scale products and are important in making medical decisions (Bennett, Smith, & Irwin, 1999). The few existing studies of pangolin scale trade have focused only on the presence/absence of illegal scale trade or analysing illegal trade reports, which revealed important findings such as the widespread availability of illegal products in TCM markets and key transit cities along illegal trading routes (Cheng, Xing, & Bonebrake, 2017; Xu et al., 2016; Yin et al., 2015). However, knowledge and attitudes of TCM practitioners about pangolin scale medicines are also crucial for regulating pangolin scale trade, since this stakeholder group has the potential to influence consumer behaviours and decide or guide consumption (Doughty et al., 2019; Tan & Freathy, 2011).
Based on these key gaps in the knowledge of the pangolin trade, we aim to provide new insights into how TCM practitioners and other TCM-related stakeholders (sellers and the general public) in two provinces in China understand and view this trade. We hypothesise that practitioners and other key stakeholders may not fully understand the legality and conservation impacts of pangolin trade, which might influence their attitude and consequently their behaviour. The insights gained through this approach should enable more effective identification of possible interventions that can provide essential information for TCM-related stakeholders to support effective pangolin conservation and better control of legal scale trade.
2 MATERIALS AND METHODS
Between October 2016 and April 2017, we conducted interviews to collect information on knowledge about, and attitudes towards, trade in pangolins and pangolin scale products in TCM in nine administrative regions across two Chinese provinces: Henan Province (Kaifeng, Yuzhou and Zhengzhou municipalities) and Hainan Province (Baisha, Haikou, Ledong, Qiongzhong, Sanya and Wuzhishan counties; Figure 1). These provinces were chosen because we had access to readily available local contact networks in both regions. Furthermore, Henan and Hainan also vary greatly in terms of local culture, economy, human population, topography and geographical location (National Bureau of Statistics, 2020), which can increase site representation and reveal more general patterns about knowledge and attitudes across China. Our respondents included four stakeholder groups: (a) doctors currently working in hospitals (either TCM hospitals or hospitals containing TCM departments; one per hospital); (b) shop owners or assistants from TCM shops (one per shop); (c) sellers from TCM wholesale markets (one per wholesale shop) and (d) members of the general public living in urban centres (towns and cities). TCM consumers are difficult to pinpoint before interview, so we targeted the general public as potential consumers, and past consumption was queried during interviews to help identify actual consumers.

FIGURE 1
Interviews with TCM practitioners/sellers were conducted face to face in Mandarin by the lead author. We accessed doctors in both Henan and Hainan, and wholesalers and TCM shops in Henan through social connections, primarily through introduction of potential respondents by friends or family members. We tried to reach as many of these respondents as possible within the research time period with no set sample size. We accessed pharmaceutical shops in Hainan through cluster sampling, which involved use of an online map (Baidu Map, similar to Google Map) to identify areas within each county where pharmaceutical shops were concentrated, and then conducted interviews in all shops in those areas. We aimed to survey 30 shops per county or all shops present in town centres. Shops that were found not to sell TCM products were removed from analysis.
Public surveys in Henan were conducted using online snowball sampling, and questionnaires were sent out through social connections in Kaifeng and Zhengzhou using online social media including WeChat and QQ. The target sample size for each municipality was 600 and 400 respectively. Public surveys in Hainan were conducted face to face in Mandarin by the lead author and local volunteers using street encounter sampling. Locations of streets were selected to cover a wide geographic spread and include diverse functional sites to maximise representation in the sample by including people with diverse socio-economic backgrounds. The target sample sizes were 200 for Haikou and Sanya, and 100 for other counties. Online snowball surveys were also attempted in Hainan but had a low participation rate, and so were excluded from analysis.
During public surveys, responses were entered directly into the Wenjuanxing survey platform (https://www.wjx.cn/) by respondents or with assistance from interviewers if needed. The age and gender structure of respondents were monitored during the survey to compare with the known age and gender structure of each province (Henan Provincial Bureau of Statistics, 2016; National Bureau of Statistics, 2011). Age and gender groups with lower proportions of respondents compared with the provincial population structure were targeted to recruit more respondents and improve representativeness of the overall sample. To increase participation rates, we offered tokens of thanks to potential participants costing around 0.1 USD each, comprising cotton towels in street surveys, and red bags in online snowball surveys.
We developed two Chinese language question lists targeting TCM practitioners/sellers and the general public respectively (see Supporting Information). The interview targeting TCM practitioners/sellers was semi-structured and focused on four aspects of pangolin scale trade, both legal or illegal: (a) demand for pangolin scale medicine, including commonly targeted symptoms and whether medicinal substitutes exist; (b) related legislative or institutional regulations that they were aware of; (c) knowledge and attitudes towards pangolin scale trade (knowledge includes trade volume and product price and their long-term or seasonal fluctuations, and source of products; attitude refers to supportiveness towards trade) and (d) knowledge about pangolins, such as conservation status or any ecological knowledge. Each interview took 10–30 min to complete. The public survey used a set questionnaire focused more on the latter three topics, with most questions in multiple choice format, and which took 10 min on average to complete. Project design was approved by the Department of Geography Ethics Review Group, University of Cambridge (#1503). All respondents were kept anonymous and only respondents who provided oral or written consent were included in the study.
The question lists produced both quantitative and qualitative data. Quantitative data were analysed in RStudio with z-tests to compare proportions and binomial logistic regression to understand factors affecting the public’s supportiveness towards trading pangolin medicine, with binomial regression models developed separately for each province (RStudio Team, 2015). Variables included in the maximal model were respondent age, gender, education, ethnic group, annual income, study area, knowledge of pangolin population status in China, knowledge of source of pangolin products in market, previous consumption of pangolin medicine, knowledge of pangolin medicine legality and knowledge of whether pangolins are protected animals. Stepwise selection was performed using stepAIC to find the best-performing model with the lowest Akaike information criterion. Coefficients for variables in the model were standardised using beta to identify the most influential factor. Qualitative data were analysed using content analysis (Newing, Eagle, Puri, & Watson, 2010). Responses to open-ended questions were coded according to response type, codes were grouped into categories that formed clusters and cluster patterns were identified to describe the target groups. Maps used in this study were plotted using QGIS (QGIS Development Team, 2019).
3 RESULTS
In total, we interviewed 2,301 respondents (Table 1), including doctors from 41 hospitals, 37 shop owners and 53 shop assistants from 90 TCM shops, 2,168 members of the public (1,221 in Henan, 947 in Hainan) and two sellers from TCM wholesale markets in Yuzhou and Zhengzhou (Henan) respectively.
| Province | Municipality/county | Doctors surveyed | Sellers surveyed | Members of the public surveyed |
|---|---|---|---|---|
| Henan | Kaifeng | 9 | 6 | 431 |
| Henan | Yuzhou | 0 | 1 (wholesaler) | 0 |
| Henan | Zhengzhou | 19 | 8 (including 1 wholesaler) | 790 |
| Hainan | Baisha | 1 | 11 | 117 |
| Hainan | Haikou | 4 | 24 | 226 |
| Hainan | Ledong | 2 | 7 | 119 |
| Hainan | Qiongzhong | 3 | 14 | 154 |
| Hainan | Sanya | 2 | 13 | 209 |
| Hainan | Wuzhishan | 1 | 8 | 122 |
| Total | 41 | 92 | 2,168 |
3.1. TCM practitioners and sellers
The medicinal value of pangolin scales was supported by most respondents working in hospitals (97.6%). In the 41 hospitals surveyed, only one doctor expressed uncertainty about the medicinal value of pangolin scales. However, the hospital in which this doctor worked also sold pangolin scales. Most doctors also showed a good understanding of the medicinal use of pangolin scales in TCM. Doctors from 31 hospitals (75.6%) listed specific symptoms that could be treated with prescriptions containing pangolin scales. These symptoms can be grouped into six categories (Table 2). Among the symptoms, stimulating milk secretion, mammary gland hyperplasia, infertility, liver disease and tumours were mentioned regularly by doctors from different hospitals.
| Categories | Examples |
|---|---|
| Gynaecological disorders | Infertility (caused by fallopian tube obstructions or other disorders), uterine fibroids, blockages in mammary glands, mammary gland hyperplasia, irregular menstruation, problems with milk secretion |
| Liver diseases | Tumours or swelling, cirrhosis, hepatitis B |
| Other tumours and swellings | Angiomas, rhinitis, desmoid tumours, goitre, swollen spleen, benign prostatic hyperplasia, adenoid hypertrophy |
| Symptoms related to blood circulation | Blood stasis/circulatory problems, cerebral thrombosis, vasculitis, bruises |
| Bone-related symptoms | Fractures, joint pain and rheumatoid arthritis, lumbar disc protrusion |
| Skin disorders | Acne, suppuration |
Nevertheless, while many doctors knew about the medicinal or healthcare value of pangolin scales, very few knew about regulations around pangolin products. Doctors generally had little knowledge of the legality of the pangolin scale trade or the protected status of pangolins. Only five of 41 doctors (12.2%) said that pangolins were protected animals, and only two (4.9%) said that pangolins could not be sold in the market (the term ‘market’ here may or may not include hospitals). When asked about regulations regarding the prescription and sale of pangolin scales, no doctor mentioned the permit required for legal sale of pangolin scales or the quota system. When asked about restrictions on hospital usage or stocking of scales, most doctors responded that scales were ‘stocked as needed’ or ‘prescribed as needed’. One hospital was found to ask their doctors to systematically add pangolin scales to every patient in every prescription.
Similarly, pharmaceutical shop interview results showed that only 19 of 90 respondents (21.1%) mentioned that pangolins were protected animals, and only two (2.2%) specifically mentioned that pangolin products were not allowed to be sold. Among these 19 respondents, 11 were shop owners; the reporting rate on this topic from shop owners (11 of 37, 29.7%) was higher than from shop assistants (8 of 53, 15.1%), but the difference was not statistically significant (z-test, p = 0.10).
Conversely, wholesale market sellers showed a detailed understanding of the pangolin scale trade and related regulations. The wholesaler from Zhengzhou Wholesale Market correctly reported that pangolins were listed as Class II protected animals (at the time of interview) and that pangolin scales were regulated by the government. The wholesaler from Yuzhou Wholesale Market said it was illegal to sell pangolin scales, but a lot of shops ran a hidden trade. In terms of their medicinal value, the wholesaler from Zhengzhou believed that pangolin scales could not be substituted because they were very effective even in small dosages, especially when treating tumours and liver diseases. One wholesaler and two shop owners also mentioned the widespread counterfeiting of pangolin scales in markets, including the use of fake scales made of pig or goat hoof, smoking scales with chemicals to increase their weight and including pangolin nails within scale products.
3.2. General public
The general public in Henan and Hainan generally showed little knowledge of the pangolin trade. When asked about their knowledge of pangolins, only 7.2% of respondents from Hainan and 16.9% from Henan mentioned the medicinal value of pangolins. Although most respondents in both provinces did not support trade in any pangolin products, respondents from both provinces were significantly more supportive of the trade of pangolin medicine products compared to trade for food or ornaments (z-test, p < 0.01; Figure 2).

Fig 2. Respondents’ attitudes towards trade in pangolin products for different purposes. Asterisks show ‘support’ proportions that differ significantly from each other within a province
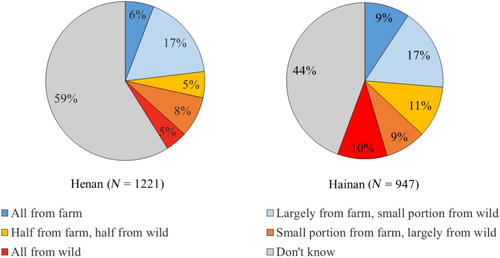
Most respondents (66.3% in Hainan, 76.2% in Henan) knew that pangolin populations in China were threatened to some degree (either Critically Endangered, Endangered or Vulnerable). However, more than 20% (25.6% in Hainan, 21.4% in Henan) were not aware of the level of threat faced by pangolins. Between 25% (Hainan) and 41% (Henan) of respondents believed that pangolin scale medicines could be traded legally. This was again significantly higher than perceptions about legality of trade for food and ornaments (z-test, p < 0.01; Figure 3). However, 44% (Hainan) and 59% (Henan) of respondents did not know the source of these products, and only 4%–10% correctly understood that all pangolin products were wild-sourced (Figure 4).
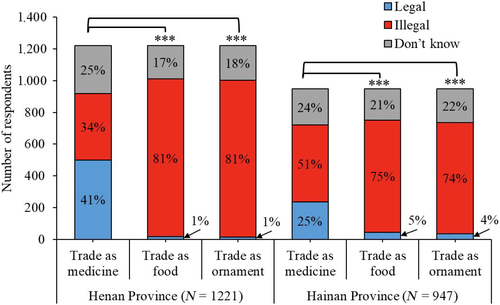
Fig 3. Respondents’ knowledge of the legality of trading pangolin products for different purposes. Asterisks show ‘legal’ proportions that differ significantly from each other within a province

Fig 4. Respondents’ knowledge about source of pangolin products sold in markets
Binomial regression model results for Henan (Table 3) show that female respondents, respondents who thought that pangolin populations were not threatened or did not know their status, respondents who work as professionals or civil servants, respondents with previous experience of consuming pangolins and respondents who thought pangolin scale medicines were legal, were significantly more likely to support trade. More highly educated respondents were also more likely to support trade, but this result was not statistically significant. Freelancers were more likely not to support the trade, but this was also not statistically significant. Hainan model results (Table 4) show that older respondents, respondents with previous experience of consuming pangolins, respondents who thought pangolin scale medicines were legal and respondents who thought pangolin products originated from farms or who did not know their origin were significantly more likely to support trade.
| Henan model | Std. Estimate | SE | z value | p value |
|---|---|---|---|---|
| (Intercept) | 0.0000 | 0.72522 | −1.816 | 0.06938 |
| Gender | −0.2833 | 0.17177 | −2.444 | 0.0145 |
| Occupation (professional) | 0.46521 | 0.30268 | 2.365 | 0.01805 |
| Occupation (civil servant) | 0.55655 | 0.35042 | 2.867 | 0.00414 |
| Occupation (freelancer) | −0.32176 | 0.28820 | −1.662 | 0.09649 |
| Education | 0.34655 | 0.18782 | 1.847 | 0.06474 |
| Pangolin population status in China | 0.37346 | 0.05607 | 2.191 | 0.02847 |
| Past consumption behaviour | 0.882595 | 0.17412 | 4.530 | 5.9e−06 |
| Medicine legality | 3.679018 | 0.11804 | 17.175 | <2e−16 |
| Hainan model | Std. Estimate | SE | z value | p value |
|---|---|---|---|---|
| (Intercept) | 0.0000 | 0.29319 | 0.915 | 0.360357 |
| Age | 0.552367 | 0.05354 | 2.443 | 0.014581 |
| Source of commodities | −0.84557 | 0.05555 | −3.798 | 0.000146 |
| Past consumption behaviour | 0.8357 | 0.17028 | 3.856 | 0.000115 |
| Medicine legality | 3.42867 | 0.12441 | 14.624 | <2e−16 |
4. DISCUSSION
Our study shows that most TCM practitioners in sampled hospitals and pharmaceutical shops across two Chinese provinces believe pangolin scales have high medicinal value. We also confirm the important role that these TCM practitioners, rather than end consumers, play in deciding consumption of medicinal pangolin scale products. Few patients questioned the use of pangolin scales in prescriptions, and if so, they asked for substitutes due to the relatively high price of scales rather than for conservation reasons. These findings highlight the need to engage more widely across the TCM community to support pangolin conservation and regulation of pangolin trade. Previous studies on the use of rhino horn, bear bile and saiga horn have also highlighted the importance of understanding and working with TCM practitioners as a key stakeholder group in trade regulation (Cheung, Mazerolle, Possingham, & Biggs, 2018; Doughty et al., 2019; Moorhouse, Coals, D’Cruze, & Macdonald, 2020; Randolph, Zhang, Tran, Nguyen, & Ha, 2019). However, few studies or conservation interventions involving Chinese TCM practitioners have been conducted or developed to date.
This previous lack of conservation targeting might help to explain our observation that doctors in hospitals and shop assistants in pharmaceutical shops possessed little knowledge of the legality of pangolin trade, since no education or awareness-raising programmes have targeted this stakeholder group. In contrast, shop owners and wholesalers were found to have a better understanding of relevant regulations. Similarly, wholesalers in China have been shown to be more aware of the illegal nature of saiga horn trade and more cautious about openly discussing the topic than retailers (Li, Zhao, & Bennett, 2007). These observations probably reflect the fact that conservation interventions have so far focused more on upstream sellers/manufacturers (TRAFFIC, 2015; Xu et al., 2016). Future conservation programmes should therefore also target other end sellers to improve their awareness of relevant legislation and conservation information about pangolins. Without this knowledge, these important decision makers will not be able to make informed choices to avoid or refuse illegal products.
The results from our public survey revealed that the sampled general public has little understanding of the source of pangolin products (Figure 4). Many respondents did not know where these products came from, while some believed that pangolin products were obtained from farmed animals. Awareness of the source of pangolin products was also found to be an influential factor that correlated with people’s attitude towards the trade in our regression model for Hainan (Table 4). This finding further highlights the need for targeted education on the source of pangolin products, which may alter people’s attitude towards pangolin products and their subsequent behaviours. Moreover, without understanding that pangolin products are all wild-sourced and threaten the survival of wild pangolin populations, the causal relationship between products sold in markets and conservation of threatened wild pangolins will not be appreciated.
Our models show that awareness of the legality of pangolin products was the strongest factor influencing people’s supportiveness towards pangolin medicine in both provinces, as suggested by the highest standardised coefficient in our regression models (Tables 3 and 4). This finding suggests that improving conservation awareness around legality of the trade might produce a more uniform and stronger positive impact on reducing demand for illegal pangolin products compared to other educational topics, such as awareness raising about wild pangolin population status, since other such factors have a weaker effect or are not significant in our regression models. Improving awareness of legality is also highlighted as an important activity by the lack of evidence in our study to suggest that the public can differentiate accurately between legal versus illegal pangolin scale products. Indeed, the opposite conclusion is indirectly supported by our observation that end sellers, who are often the key decision makers for pangolin scale consumption, lacked knowledge on relevant regulations.
More positively, our study shows the feasibility of encouraging TCM practitioners to use substitutes to replace pangolin scales. More than 70% of doctors that we interviewed agreed that at least some current use of pangolin scales in TCM could be substituted by other ingredients. This finding is supported by previous studies that compared the medicinal effect of pangolin scales with other TCM ingredients such as pig hoof and different plant products (Burgess, Olmedo, Veríssimo, & Waterman, 2020; Ge, Tong, Qin, Li, & Gao, 2009; Li, Zhao, Chen, & Hou, 2008; Xing et al., 2020; Zhang, Tong, Gao, & Li, 2009). Most of the potential substitutes are from domesticated or cultivated species and are thus unlikely to be of conservation concern. However, there is still a need to evaluate the potential impacts to wild populations if the demand for substitutes is likely to increase (Phelps, Carrasco, & Webb, 2014).
Traditional Chinese Medicine communities could switch to other more sustainable substitutes if sufficiently motivated. One motivation for TCM doctors to use substitutes for pangolin scales could be caring for the well-being of their patients. Since the quality of illegal or counterfeit products cannot be guaranteed, the fact that illegal and counterfeit pangolin scale products are widespread in markets could therefore help motivate TCM practitioners to reconsider their choice of prescription (Xu et al., 2016; Yin et al., 2015). Two recent changes in policy might promote practitioners to actively consider using substitutes for pangolin scales if they are made aware of these changes.
Firstly, the National Healthcare Security Administration and the Ministry of Human Resources and Social Security (2019) recently updated the ‘National Drug Catalogue for Basic Medical Insurance, Work-Related Injury Insurance, and Maternity Insurance’, and pangolin scales were removed from this catalogue. This means pangolin scales are no longer covered by national health insurance, meaning that practitioners might now actively consider substitutes to help reduce patients’ medical expenses. Moreover, in early June 2020, all Asian pangolin species (Manis spp.) were uplisted from Class II to Class I national-level protection in China, and pangolin scales were removed from the official list of Chinese Pharmacopoeia due to the heavily threatened status of wild pangolin populations (National Pharmacopoeia Committee, 2020). This national policy change means that pangolin scales should no longer be regarded as an authorised medicine, although the ingredient is still present in some of the patent drugs included in the pharmacopoeia, and the legal pangolin scale market has not been closed. However, this removal could still serve as a strong signal to the TCM community that legal usage of pangolin scales might end in the near future and make exploration of effective substitutes a more pressing issue than before. Therefore, targeted education or awareness-raising programmes focusing on regulations and current market status might facilitate TCM practitioners to participate willingly in pangolin conservation by refusing illegal pangolin products and choosing sustainable substitutes when possible.
The use of pangolin scales as a general healthcare product (in contrast to a specific medicinal product or prescription) was not acknowledged by TCM doctors from hospitals in our survey. This alternative potential use is also not acknowledged by the National Health Commission of China in their official list of 114 TCM ingredients that can be used for non-medicinal uses or for general healthcare (National Health Commission of China, 2002), which does not contain pangolin scales or other pangolin products. TCM practitioners, rather than conservationists, are seen by the Chinese public as authorities in the healthcare domain (Burgess et al., 2020; Si, Song, & Gao, 2013), and so demand reduction campaigns should consider inviting authorities from the TCM community to speak out to guide demand. As such, TCM practitioners are important stakeholders who are currently underrepresented in pangolin conservation, but who have the ability to lead the public towards a more sustainable lifestyle.
Finally, it is important to recognise some limitations of this study. The failure of snowball online surveying in Hainan led to our use of different sampling methods in the two study provinces. In addition to differences in knowledge of pangolin population status and source of products between the two regression models, the Henan model highlighted female respondents and respondents working as professionals or civil servants whereas the Hainan model highlighted older respondents as more likely to support trade. Although these province-level differences suggest that conservation campaigns might need to be regionally modified to accommodate local variation (Olmedo, Sharif, & Milner-Gulland, 2018; Wallen & Daut, 2018), they might also be due to our different sampling methods rather than underlying regional differences in attitudes and awareness. Secondly, only certain administrative regions in each province were surveyed, and our sample size is inevitably low compared to the total population living in each region. For reference, the population of Kaifeng is 2 million, the population of Zhengzhou is 7 million and the population of Baisha (the least populous region included in our study) is 30,000. Assessing the representativeness of the patterns seen in our study across wider demographic and geographical scales therefore needs further validation. Thirdly, although knowledge and attitudes of direct consumers are important to understand for trade regulation, individuals belonging to this stakeholder group are hard to pinpoint and underreporting is common in self-reporting surveys such as ours (Krumpal, 2013). This study therefore represents an assessment of people who currently support the pangolin TCM trade, rather than those who specifically report past experience of consuming pangolins. However, it is possible that factors influencing support towards trade may differ from those influencing actual consumption of products. To be successful at effecting behaviour change, campaigns that aim to change consumption may therefore need to be based on further evidence. Moreover, only two wholesalers were interviewed, one from each wholesale market. Although these respondents showed a good understanding of the wholesale market they worked in, a greater sample size is definitely required to understand knowledge and attitudes of this stakeholder group.
Despite the potential caveats of the study, our results suggest three potential directions for future interventions to support pangolin conservation in China. Firstly, awareness and education programmes should focus more on end sellers and their lack of understanding about relevant regulations and the illegal market. As key decision makers in pangolin scale consumption, their knowledge on product legality links closely with trade management on the ground. Secondly, interventions that target the general public should highlight the connection between products in markets and populations of wild pangolins, and combine these perspectives with practical guidelines on what the public could do to participate effectively in combating illegal trade and reducing demand on pangolin products. These guidelines could include how to identify and report illegal products, how to identify pangolin scale ingredients in prescriptions and the importance and feasibility of actively consulting TCM practitioners for potential substitutes. Audience segmentation is preferred for public campaigns when possible, and our results suggest more localised segmentation might be needed. Thirdly, the TCM community should be recognised as a key stakeholder in pangolin trade and become more closely integrated into pangolin conservation activities. The role of TCM practitioners as healthcare professionals could help to reduce excessive and illegal demand not only on pangolins but potentially also on many other wildlife products. Therefore, we strongly urge that the TCM community should become more heavily involved in future efforts to conserve pangolins and other wildlife threatened by unsustainable medicinal trade.
Source: British Ecological Society

{kind=link}
{kind=link}